Trends of Pacemaker Implantation in the United States:

Pacemaker Use in the United States From 1993 Through 2009
The most common type of pacemaker used in the United States is the dual chamber pacemaker while the implantation rate of single atrial pacemakers has always been at a low. Biventricular pacemakers were introduced in 2002 and the rate of implantation has remained fairly low. Single ventricle pacemakers, on the other hand, have been on a steady decline although they are more common than both single atrial and biventricular pacemakers. (Greenspoon et al., 2012, 1540-1545).

Average Age of Pacemaker Patients at Time of Implantation
The average age of patients requiring pacemakers has been constantly increasing over time. Patients with single ventricular devices are older than those with dual chamber pacemakers. In general, the youngest need single atrial pacemakers and the average age of patients with biventricular devices is slightly less than those with dual chamber pacemakers. (Greenspoon et al., 2012, 1540-1545).
The average age of patients requiring pacemakers has been constantly increasing over time. Patients with single ventricular devices are older than those with dual chamber pacemakers. In general, the youngest need single atrial pacemakers and the average age of patients with biventricular devices is slightly less than those with dual chamber pacemakers. (Greenspoon et al., 2012, 1540-1545).

|
Hospital Charges Associated With Permanent Pacemaker Implantation From 1993 Through 2009
The hospital charges associated with pacemaker implantation has been constantly increasing over time, with the implantation of biventricular pacemakers being the most costly for patients. (Greenspoon et al., 2012, 1540-1545). |
Complications Associated with Pacemaker Implantation:
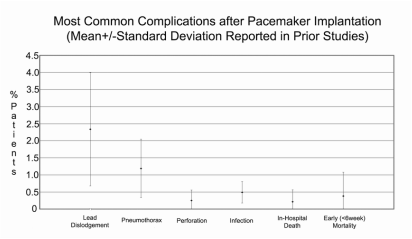
In this study done by researchers at Selcuk University, within 30 days of pacemaker implantation, about 4-7% of the patients developed complications. These complications included lead dislodgement (a position change of the pacemaker resulting in malfunctioning (Fuertes, Toquero, Arroyo-Espliguero, & Lozano, 2003, 231-238)), pneumothorax (a collapsed lung that occurs during the subclavian vein puncture (Gul & Kayrak, 2011)), perforation (a hole in the heart caused by the leads of the pacemaker (Banaszewski & Stępińska, 2012, 11-13)), and infection as well as in-hospital death and early mortality. The most common complications are lead dislodgement and pneumothorax while perforation, infection, in-hospital death, and early mortality are less frequent. (Stevenson & Williams, 2012).
Clinical Study on Improvement with Pacemakers:


|
A study was done on patients with Biorate and Meta pacemakers to see if there was an improvement in exercise duration due to the pacemaker. Patients were given treadmill exercise tests and exercised until they were breathless or fatigued. Results show that there was a significant improvement in the exercise duration of both groups of patients. There was a 29% improvement among the patients with a Biorate pacemaker and a 32% improvement among the patients with a Meta pacemaker. The study also investigated whether there was a correlation between pacing rate and oxygen consumption. In the Biorate group, there was a correlation of 0.81 and in the Meta group, there was a correlation of 0.83. All these results show that both pacemakers, Biorate and Meta, had significantly positive effects on the patients. ("Single-chamber Cardiac Pacing with Two Forms of Respiration-controlled Rate-responsive Pacemaker: Statistics", 2014).
|
References:
Banaszewski, M., & Stępińska, J. (2012). Right heart perforation by pacemaker leads. Archives of Medical
Science, 8(1), 11-13.
Fuertes, B., Toquero, J., Arroyo-Espliguero, R., & Lozano, I. (2003). Pacemaker Lead Displacement:
Mechanisms And Management. Indian Pacing and Electrophysiology Journal,3(4), 231-238.
Greenspon, A., Patel, J., Lau, E., Ochoa, J., Frisch, D., Ho, R., ... Kurtz, S. (2012). Trends in Permanent
Pacemaker Implantation in the United States From 1993 to 2009. Journal of the American College of
Cardiology, 60(16), 1540-1545.
Gul, E., & Kayrak, M. (2011). Common Pacemaker Problems: Lead and Pocket Complications. In M. Das
(Ed.), Modern Pacemakers - Present and Future. InTech.
Single-chamber Cardiac Pacing with Two Forms of Respiration-controlled Rate-responsive Pacemaker: Statistics. (2014, October
13). Retrieved November 29, 2014, from http://www.depressionofspirits.com/single-chamber-cardiac-pacing-with-two-
forms-of-respiration-controlled-rate-responsive-pacemaker-statistics-3302.html
Stevenson, R., & Williams, J. (2012). Complications of Pacemaker Implantation. In A. Roka (Ed.), Current
Issues and Recent Advances in Pacemaker Therapy. InTech.
Science, 8(1), 11-13.
Fuertes, B., Toquero, J., Arroyo-Espliguero, R., & Lozano, I. (2003). Pacemaker Lead Displacement:
Mechanisms And Management. Indian Pacing and Electrophysiology Journal,3(4), 231-238.
Greenspon, A., Patel, J., Lau, E., Ochoa, J., Frisch, D., Ho, R., ... Kurtz, S. (2012). Trends in Permanent
Pacemaker Implantation in the United States From 1993 to 2009. Journal of the American College of
Cardiology, 60(16), 1540-1545.
Gul, E., & Kayrak, M. (2011). Common Pacemaker Problems: Lead and Pocket Complications. In M. Das
(Ed.), Modern Pacemakers - Present and Future. InTech.
Single-chamber Cardiac Pacing with Two Forms of Respiration-controlled Rate-responsive Pacemaker: Statistics. (2014, October
13). Retrieved November 29, 2014, from http://www.depressionofspirits.com/single-chamber-cardiac-pacing-with-two-
forms-of-respiration-controlled-rate-responsive-pacemaker-statistics-3302.html
Stevenson, R., & Williams, J. (2012). Complications of Pacemaker Implantation. In A. Roka (Ed.), Current
Issues and Recent Advances in Pacemaker Therapy. InTech.
